| |
|











|
|

.jpg)
|
|
|
Control your diabetes permanently with
"Insulin, Food and
After-Meal Exercise." This is what diabetes
care is all about! A trial and error procedure
was developed to determine the appropriate
insulin dose for a given amount of food consumed
followed by an after-meal exercise. The trial
and error procedure is described in a flow sheet
below.
Luckily red blood cells die every 90 days and
new red blood cells are born. So the degree of
diabetes control during the preceding 90 days
can be easily monitored and understood. Due to
lack of proper knowledge, most diabetics fail to
understand the concept of hemoglobin A1c and as
a result, face serious long term side effects of
uncontrolled diabetes
and die. If a diabetic person understands the lifespan
of red blood cells, the purpose of hemoglobin
A1c test thoroughly,
and how the hemoglobin A1c chart was designed by
medical scientists, then he/she can permanently control diabetes and
live like a normal person forever thereafter.
Diabetes Breakthrough:
A
new diabetes control treatment illustrated in
this book "Permanent Diabetes Control" lowered blood
glucose levels after eating, stabilized the
average blood glucose level, caused the hemoglobin
A1c level to drop from a high risk 12% to a
stunning 6.2%, and then to an amazing 5.0%, and reversed
critical heart disease without bypass surgery.
|
|
|
|
|
How To Control Type 2 Diabetes Permanently
How To
Control Type 1 Diabetes Permanently
By Slashing After-Meal Blood Glucose Spikes |
|
Many people with diabetes focus their attention
on fasting glucose levels in order to control
diabetes, rather than on lowering after-meal
glucose levels. If your blood glucose level from
a finger-stick blood test early in the morning
is normal, it doesn't mean your diabetes is
controlled. Hemoglobin A1c is a parameter
that directly reveals the degree of "diabetes
control" during the preceding 90 days. Red blood
cells live in the bloodstream 60 to 90 days.
Every 90 days, new red blood cells are born. Hemoglobin is a protein molecule that carries
and supplies oxygen from the lungs to the trillions of body's
cells wherever it is needed. While the blood
circulates, depending on how high or how low the blood
glucose level is, a certain amount of glucose is
attached to the hemoglobin molecules to form
glycated hemoglobin. Different people call it with different
names: glycated A1c, hemoglobin A1c (HbA1c), or simply A1c. Therefore, by
measuring the hemoglobin A1c level in a
laboratory from the patient's blood sample, it is possible to know
the average blood glucose level and the degree
to which it has been controlled over the
preceding 90 days. Which obviously means that it
takes at least 90 days to see any significant improvement in
the hemoglobin A1c level from a laboratory
blood test.
Blood glucose reaches its highest level immediately after a major meal
consumption. The elevated glucose levels
dominate and largely contribute to establishing the average
glucose level over 90 days. After-meal glucose levels therefore
must be slashed immediately after eating, lowered and brought to normal within 1 or 2 hours of the
consumption of every major meal consumption in order to
control and lower hemoglobin A1c close to its normal value.
At the same time, the insulin dose must be optimized.
Too much insulin causes hypoglycemia and constricts arteries,
leading to heart attack and coronary heart disease. Too much
insulin also stimulates the brain to feel hungry
and eat more and causes the liver to manufacture fat in the
belly. Too little insulin on the other hand would not be enough
to cover the entire meal, suggesting the fact that there must be
an optimal insulin dose. Insulin is
synthesized in such a way that it acts more quickly and much
more effectively with any type of physical activity or exercise. After-meal exercise,
either treadmill, bike or regular walking, should be introduced into the
diabetes control plan in order to burn fat, lose calories and
optimize both the insulin dose and insulin action. After-meal
exercise minimizes the insulin dose and maximizes insulin action
and prevents after-meal glucose levels from rising too high,
thus keeping diabetes under tight control.
The Good News:
Consistent, serious and rigorous efforts towards lowering
after-meal glucose levels over a period of 3 to 6 months
gradually lowers the hemoglobin A1c level of a diabetic person
to its normal value, even if the diabetes was poorly controlled
in the past. Thereafter, continued efforts with a
reasonable attention to Insulin, Food and
After-Meal Exercise
are necessary to permanently control diabetes.
The author of this book (Dr. RK), having been a seriously diabetic
person (a highly insulin-dependent diabetc person), began conducting
diligent experiments to study the combined influence of insulin
and after-meal exercise on after-meal blood glucose levels, and
successfully lowered his after-meal glucose levels continuously
and on a daily basis. For a selected major high-carbohydrate meal (either
the lunch or evening
meal/supper), the Humalog insulin dose was cut by 50 to 60%
through extensive research and optimization. The official
blood tests indicated that hemoglobin A1c level dropped quickly
in a short period of time from a
very high-risk 12% to a stunning 6.2%, and then trended towards
5.0%, and since then has
remained steady and normal (under or close to 6.0 %) till now, indicating that the
diabetes has been permanently controlled. Shown below is the
flowsheet of the trial and error procedure Dr. RK developed and
used successfully to control diabetes in order to find out the optimal insulin dose for
any given high-carbohydrate meal.
Dr. RK
Controlled His Diabetes Permanently, and
Reversed His Critical
Diabetic Heart Disease
Without Any Bypass Surgery
During 1998-99, the participant of this diabetic research (Dr.
RK) suffered from severe angina, and
could not walk even a block as his heart arteries were clogged.
It was clear that he was suffering from a critical heart
disease. An Angiogram indicated that his left artery was
75% clogged, and his cardiologist recommended and insisted an
immediate bypass surgery. But Dr. RK said "NO" to surgery, and
started controlling his diabetes diligently through conducting
daily experiments by monitoring and controlling blood glucose
levels using a glucometer at home. By conducting daily
experiments of diabetes control diligently, with healthy meal,
multiple insulin shots and exercise, he was able to successfully lower his hemoglobin A1c
levels to perfectly normal, and maintained the normal hemoglobin A1c
levels. As a result, he was able to reverse his coronary
critical heart
diseases without surgery. He has no more angina as his arteries
were cleared or unclogged.
After the completion of his research phase, as he was rewarded
by his own monitoring and researching experience, the same
participant skilfully monitors his diabetes blood glucose level
only a few times a day. He eats his favorite high-carbohydrate
meal including the dessert in restaurants once or twice a week, and yet his diabetes is
perfectly controlled. He is confident and certain that he will
be able to keep his diabetes under tight control this way for the rest of his life,
indicating that he accomplished " permanent
diabetes control."
|
|
|
Official Blood Text Results of Dr. RK
Fasting Glucose and A1c Test Results of
Dr. RK
Below
7% of HbA1c means that the diabetes is fairly controlled (for
diabetic people).
Below 6.2% of HbA1c means that the diabetes is perfectly controlled
(for
non-diabetic or healthy people).
Normal A1c for
healthy non-diabetic people: 4.5% - 6.2%
Dr. RK, in spite of being seriously diabetic person and highly
insulin-dependent,
achieved an A1c of 5.0%
with his own diligence and expert knowledge on diabetes.
Perhaps he is the only diabetic person living in this world with
permanent diabetes control!
Listed below
are the official blood test results of Dr. RK, performed with a physician’s
requisition,
by
BC Biomedical Laboratories (Life Labs), Vancouver, British
Columbia, Canada.
This table shows the evidence of how Dr. RK accomplished
Permanent Diabetes Control.
|
|
Date
|
Fasting Glucose
|
Fasting Glucose
|
Hemoglobin A1c
|
|
Units
|
mmol/L
|
mg/dL
|
g/g Hgb (%)
|
|
Normal
|
(3.6 - 6.1)
|
(65 – 110)
|
4.5% - 6.2%
|
|
|
|
|
|
|
11-Jun-1997
|
|
|
12.0%
|
|
18-Mar-1998
|
Suffered Heart Attack
(not controlled until 1998)
|
|
01-Apr-1998
|
Started controlling diabetes
(not seriously).
|
|
21-Apr-1998
|
9.2
|
165.6
|
9.6%
|
|
26-Oct-1998
|
5.7
|
102.6
|
8.0%
|
|
22-Jan-1999
|
6.0
|
108.0
|
8.4%
|
|
05-May-1999
|
5.1
|
91.8
|
8.1%
|
|
07-Jun-2000
|
7.0
|
126.0
|
10.2%
|
|
07-Jun-2000
|
Started controlling diabetes seriously.
|
|
01-Aug-2000
|
6.0
|
108.0
|
8.2%
|
|
19-Sep-2000
|
5.6
|
100.8
|
7.4%
|
|
|
|
|
|
|
19-Jan-2001
|
4.9
|
88.2
|
6.6%
|
|
29-Nov-2001
|
5.2
|
93.6
|
6.5%
|
|
05-Mar-2002
|
5.2
|
93.6
|
6.6%
|
|
06-May-2002
|
4.9
|
88.2
|
6.5%
|
|
26-Jun-2002
|
4.4
|
79.2
|
6.6%
|
|
02-Oct-2002
|
4.0
|
72.0
|
6.3%
|
|
30-Jan-2003
|
5.1 |
91.8
|
6.2%
|
|
08-Apr-2003
|
4.7 |
84.6
|
6.2%
|
|
|
|
|
|
|
03-Aug-2011
|
4.9
|
88.2
|
6.0%
|
|
01-Nov-2011 |
3.9 |
70.2 |
5.8% |
|
|
|
|
|
|
01-Feb-2012 |
3.9 |
70.2 |
5.5% |
|
01-May-2012 |
4.4 |
79.2 |
5.5% |
|
01-Aug-2012 |
3.7 |
66.7 |
5.5% |
|
23-Oct-2012 |
4.1 |
73.8 |
5.5% |
|
|
|
|
|
|
17-Jan-2013 |
4.3 |
77.4 |
5.3% |
|
01-May-2013 |
2.9 |
52.2 |
5.6% |
|
21-Aug-2013 |
5.1 |
91.8 |
5.5% |
|
|
|
|
|
|
02-Jan-2014 |
4.2 |
75.8 |
5.8% |
|
01-Apr-2014 |
4.0 |
72.0 |
5.9% |
|
02-Jul-2014 |
4.7 |
84.8 |
5.7% |
|
01-Oct-2014 |
3.6 |
64.8 |
5.5% |
|
|
|
|
|
|
02-Jan-2015 |
4.9 |
88.2 |
5.4% |
|
01-Apr-2015 |
4.7 |
84.8 |
5.4% |
|
03-Jul-2015 |
5.3 |
84.8 |
5.6% |
|
01-Oct-2015 |
4.1 |
73.8 |
5.8% |
|
|
|
|
|
|
02-Jan-2016 |
5.7 |
102.6 |
5.8% |
|
01-Apr-2016 |
4.4 |
79.2 |
5.6% |
|
02-Jul-2016 |
5.5 |
99.0 |
5.9% |
|
01-Oct-2016
|
5.3
|
95.4
|
5.0%
Personal Best |
|
05-Jan-2017 |
5.1 |
91.8 |
5.6% |
|
02-Apr-2017 |
5.5 |
99.0 |
5.4% |
|
02-Jul-2017 |
4.5 |
81.0 |
5.6% |
|
02-Oct-2017 |
4. 0 |
72.0 |
6.0 % |
|
|
|
|
|
|
Date
|
Fasting Glucose
|
Fasting Glucose
|
Hemoglobin A1c
|
|
Units
|
mmol/L
|
mg/dL
|
g/g Hgb (%)
|
|
Normal
|
(3.6 - 6.1)
|
(65 – 110)
|
4.5% - 6.2%
|
|
|
|
|
|
|
02-Jan-2018 |
4.2 |
75.6 |
5. 7% |
|
03-Apr-2018 |
4.8 |
86.4 |
5.9% |
|
02-Jul-2018 |
4.6 |
82.8 |
5.7% |
|
01-Oct-2018 |
3.4 |
61.2 |
5.7% |
|
|
|
|
|
|
02-Jan-2019 |
4.7 |
84.8 |
5.5% |
|
01-Apr-2019 |
3.9 |
70.2 |
5.6% |
|
30-Jun-2019 |
4.1 |
73.8 |
5.5% |
|
01-Oct-2019 |
4.8 |
86.4 |
5.6% |
|
|
|
|
|
|
01-Apr-2020 |
5.4 |
97.2 |
5.7% |
|
30-Jun-2020 |
3.6 |
64.8 |
5.8% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Go to the Top |
|
|
|
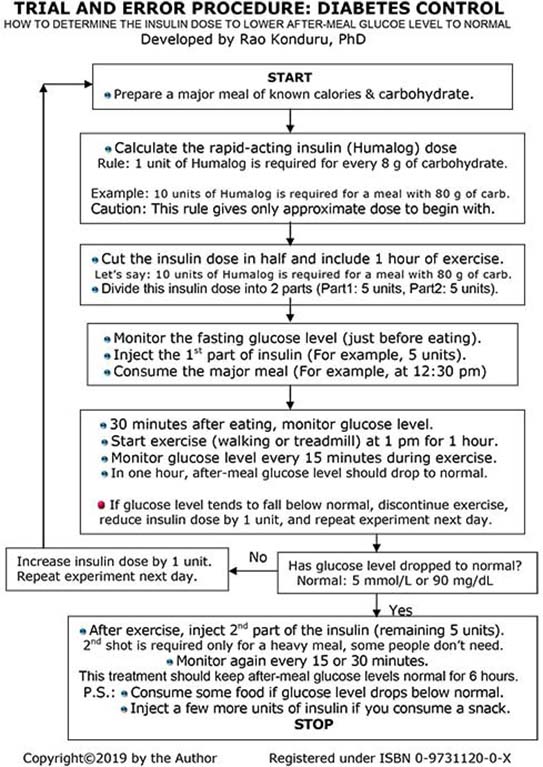
Diabetes Breakthrough In Finding Out
OPTIMAL INSULIN DOSE
Trial and Error
Procedure: Diabetes Glucose Control
Too much insulin
causes low blood sugars and hypoglycemia in a diabetic person, and constricts arteries
leading to heart
attack and/or coronary heart disease. Too much insulin also
stimulates the brain
to feel hungry and eat more, and causes the liver to manufacture
fat in the belly.
Too little insulin on the other hand would not be enough to
cover the entire meal,
suggesting the fact that there must be an optimal insulin dose
for any given meal.
The following Trial & Error Procedure has been successfully used to determine
the optimal insulin dose for any given
high-carbohydrate meal.
Dr. RK has successfully used the following Trial and Error
Procedure, and
accomplished
"permanent
diabetes control" in a very short
period of time!
|
|
If this flowsheet
is not visible clearly, read the PDF file.
click here |
|
|
 |
|
Type 2 Diabetes
Control Treatment,
Type 1 Diabetes Control Treatment, and
Treatment of Heart Disease
With Healthy Diet, Oral Medication or Insulin Shots, and After-Meal Exercise!
A
Revolutionary Approach to Control Diabetes permanently!
Permanent diabetes control is the ultimate solution to treat
chronic diabetes,
and to live like a normal person forever! |
|
Go to the Top |
|
|
.jpg)